Clonal Hematopoiesis of Indeterminate Potential is Associated with Acute Kidney Injury.
medRxiv [Preprint]. 2023 May 17:2023.05.16.23290051.
クローン性造血(CH)とAKI=急性腎障害が関連しているという論文。
過去にもCKD=慢性腎臓病とCHが関連しているという論文はあった。 Kestenbaum, B. et al. Clonal hematopoiesis of indeterminate potential and kidney function decline in the general population. Am. J. Kidney Dis. 81, 329–335 (2023). Dawoud, A. A. Z., Gilbert, R. D., Tapper, W. J. & Cross, N. C. P. Clonal myelopoiesis promotes adverse outcomes in chronic kidney disease. Leukemia 36, 507–515 (2022). Vlasschaert, C. et al. Association of clonal hematopoiesis of indeterminate potential with worse kidney function and anemia in two cohorts of patients with advanced chronic kidney disease. J. Am. Soc. Nephrol. 33, 985–995 (2022).
筆者らはまず人を対象としたいくつかのコホートでAKIとCHの関連を調査→CHを有するとAKIリスクが高いことが判明。例えば、 CHIP was associated with a 20% greater risk of AKI in a meta-analysis of these two cohorts. ※ここでのtwo cohortは the Atherosclerosis Risk in Communities (ARIC) cohort and the Cardiovascular Health Study (CHS).
Site-directed mutagenesis involves the use of primer sequences that anneal to a template DNA sequence, targeting a desired area for mutation. Polymerase chain reaction (PCR) methods allow for amplification of genomic targets in sufficient numbers for transformation.
This protocol uses MilliporeSigma's KOD Xtreme™ Hot Start DNA Polymerase, which allows for high fidelity PCR using a simple three-step thermocycle. It is important to complete the entirety of this protocol in one go, rather than delay performing the PCR, digestion, or transformation. From beginning to end, site-directed mutagenesis using this protocol can be completed in approximately 5 hours, with results from the transformation immediately available the next day.
After PCR, DpnI digestion cleaves any plasmids with methylated sites. This selects for the mutated plasmids (which are unmethylated) by destroying any remaining template DNA that were not mutated in the PCR. The DpnI from NEB is designated as a Time-Saver™ restriction enzyme that can sufficiently digest the PCR product in 15 minutes. However, it is safe to digest for longer periods of time and an incubation period of 1 hour is recommended for this protocol.
In mutagenesis, the final mutated plasmid after PCR and DpnI digestion is generally low in concentration. Therefore, high-efficiency transformation methods must be used with ultra-competent DH5α cells to achieve colonies containing the desired plasmid. The entirety of the PCR product should be used when mixing with the competent cells, and SOC medium is highly recommended for all components of the transformation (outgrowth and plate) over LB medium. Additionally, although high-throughput transformation protocols allow for some steps to be skipped, it is recommended that both heat shock and outgrowth in SOC medium are performed for mutagenesis.
This step should be performed in a cold room or on ice. For each reaction, combine the following in a PCR tube (adjust Milli-Q® water volume to compensate for template DNA concentration as necessary):
Component
Volume
KOD Xtreme™ Buffer, 2X
25 μL
Autoclaved Milli-Q® water
10 μL
dNTPs, 2 mM
10 μL
Template DNA, 25 ng/μL
2 μL
Forward primer
1 μL
Reverse primer
1 μL
* KOD Xtreme™ Hot Start DNA Polymerase, 1.0 U/μL
1 μL
Total Volume
50 μL
* NOTE: Always add the KOD Xtreme™ Hot Start DNA Polymerase as the last component, immediately before use in thermocycler. Keep the polymerase in the freezer until needed.
Spin the PCR tube in a mini centrifuge for 2–3 seconds. Do NOT spin at high rpm—only enough to ensure the polymerase is evenly mixed in.
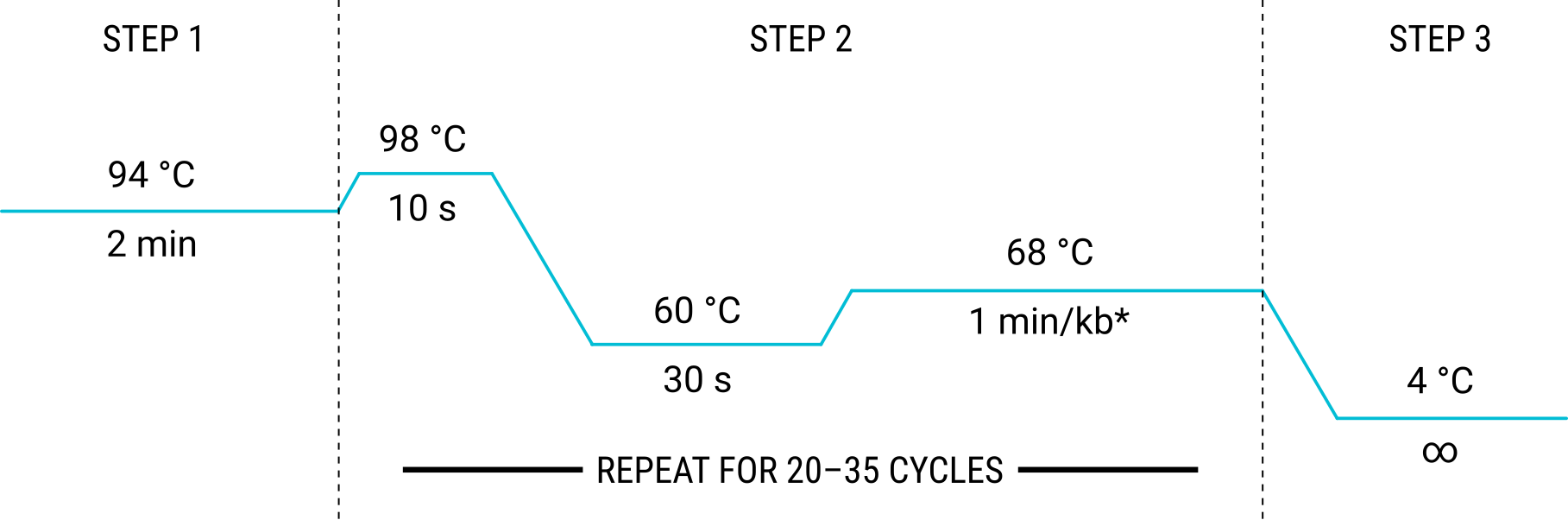
Set the thermocycler for the following cycles:
* NOTE: Adjust time according to the length of the template DNA.
Set the lid temperature to 105 °C and the reaction volume to 50 μL.
Start the run. The PCR run should take approximately 30 mins per kb of template DNA (e.g. a 6 kb plasmid template will require about 3 hours for PCR).
DpnI digestion
Add 5 μL of CutSmart® Buffer directly to the PCR product.
Add 1 μL of DpnI restriction enzyme.
Spin the PCR tube in a mini centrifuge for 2–3 seconds. Do NOT spin at high rpm—only enough to ensure the enzyme is evenly mixed in.
Incubate the PCR tube in a thermocycler at 37 °C for at least 15 minutes.
High-efficiency transformation
Thaw competent DH5α cells on ice for approximately 5–10 minutes.
Add all of the PCR product to the competent cells tube. Mix by gently tapping the side of the tube. Do NOT vortex or pipette the mix.
Incubate on ice for 10–15 minutes.
Heat shock the cells in a 42 °C water bath for 40–45 seconds.
Immediately place cells on ice for 2 minutes.
Add 500 μL of SOC media to the tube.
Incubate the cells at 37 °C while shaking at 250 rpm for 1 hour.
Spread contents of the entire transformation tube on an SOC media plate containing the appropriate antibiotic. Incubate at 37 °C for 16–18 hours.
TROUBLESHOOTING
If there are issues with mutagenesis, try the following troubleshooting tips:
Run a small amount of PCR product (~10 μL) on an agarose gel. If primer dimerization is favored over primer–template annealing, reduce the concentration of primers in the initial PCR reaction.
Check primer sequences to ensure they are complementary to the desired target on the template DNA strand.
Increase the number of cycles (max. 35) in Step 2 of the PCR.
国際他施設試験の結果は2018年NEJM発表。 Mateos MV, et al. Daratumumab plus Bortezomib, Melphalan, and Prednisone for Untreated Myeloma. N Engl J Med. 2018 Feb 8;378(6):518-528.
移植非適応患者に対するLD vd MPT: Ldの方が有意にPFS, OSともに改善する。
PFS 25.7ヵ月 vs 21.2 ヵ月 OS (4y) 59% vs 51% Benboubker L, et al. Lenalidomide and dexamethasone in transplant-ineligible patients with myeloma. N Engl J Med. 2014 Sep 4;371(10):906-17.
Len暴露あり/不応でない患者: ORR DPd 68% vs DRd 82% (有意差なし) PFS/OS中央値有意差なし
Len不応患者 ORR DPd 58% vs DRd 84% (p =0.009) PFS/OS中央値有意差なし
再発難治性骨髄腫患者に対するDKd vs Kd: OS, PFSともにDara上乗せ群で有意に延長。
1~3先行レジメン受けた患者が対象。
OS, PFSともにDara上乗せ群で有意に延長。
MRD陰性化率も高い。28% vs 9%
Saad Z. Usmani,Hang Quach,Maria-Victoria Mateos,Ola Landgren,Xavier Leleu,David Siegel,Katja Weisel,Xiaomei Shu,Chuang Li,Meletios Dimopoulos, Final analysis of carfilzomib, dexamethasone, and daratumumab vs carfilzomib and dexamethasone in the CANDOR study, Blood Adv, 2023,Usmani SZ, et al. Final analysis of carfilzomib, dexamethasone, and daratumumab vs carfilzomib and dexamethasone in the CANDOR study. Blood Adv. 2023 Jul 25;7(14):3739-3748.
KRd vs DRdのみ死亡リスク、次回治療開始のリスクが高かったが他のレジメン同士の比較では有意差なし。 Davies F, et al. Real-world comparative effectiveness of triplets containing bortezomib (B), carfilzomib (C), daratumumab (D), or ixazomib (I) in relapsed/refractory multiple myeloma (RRMM) in the US. Ann Hematol. 2021 Sep;100(9):2325-2337.
再発難治性骨髄腫患者に対するIRd vs Rd: IRdで有意に予後改善。
PFS 23.1ヵ月 vs 11.6ヵ月(p=0.001)
CR 11.1% vs 8.8%, VGPR 22.2% vs 13.9%
どちらも忍容性高く毒性は同等 Minarik, J., Pika, T., Radocha, J. et al. Survival benefit of ixazomib, lenalidomide and dexamethasone (IRD) over lenalidomide and dexamethasone (Rd) in relapsed and refractory multiple myeloma patients in routine clinical practice. BMC Cancer 21, 73 (2021).